
Photos by William DeShazer
This story originally appeared in the August 2015 issue of Louisville Magazine.
Click here to subscribe to Louisville Magazine.
The girls, they like to nod off. The boys do too. Slip into the twilight during waking hours. Teresa tells me this on a sunny June afternoon outside her boxy rental home. She’s a 49-year-old with stringy blond hair, blue eyes, and fine features that a California beach missed out on. She has lived in Austin, Indiana, her whole life.
The mother of two has a 26-year-old son in prison. Cops found nine Lorcets on him. Her daughter, Jessica, a 30-year-old whose pretty face is built as tough and square as a fist, is passed out inside — lulled by a Xanax and a half — her thick brown hair twisted into a thicket atop her head. She’s in the void, no edges or fears. Mom and daughter haven’t eaten a meal in four days. The drugs kill hunger. And they’ve got no money.
“I did two (Xanax) but I can still talk to you,” Teresa says, standing in a breezy sway. She and many others in town don’t want last names included. No one wanted to end up this way, stuck in what lately feels like spectacle. Behind her, nine dogs refuse to quiet their raspy barks. The gray mixed one chained to a tree sinks its teeth into legs as they walk away, illustrated by scabby constellations on Teresa’s calves. She can’t go to rehab with nine dogs to care for.
But Jessica wants to get clean. “Get me into rehab before I change my mind,” she’ll say to nurses, her mom, even strangers. She’s been waiting for weeks. There’s a problem with paperwork or something. So she sleeps. That way, a quarter of an Opana pill, just a quarter, just enough to satisfy the cravings in her few alert hours, can fight what lurks on the other side — the shakes that rattle so deep fingers can’t manage pen on paper, the runs never ending, an anger so hot you long to slice your own flesh. And some do. Withdrawals can kill you. Or at least, feel like they will.
Opana, a brand name for oxymorphone, is a powerful prescription opioid intended to treat chronic pain. When snorted or injected, it blasts a euphoric high. Like heroin, users feel soothed, blessed. Pain comes later. One Austin family lost both parents and a daughter within six months due to overdoses. A grandmother of 18 grandchildren can only count four who are not in state custody because of their parents’ addictions.

On the front door of their rental home in Austin, Whitney and David Ritchie have posted a sign in red ink: No knocking 9-10.
The nighttime hour is "when most of the junkies are out," David explains.
Ask anyone in Austin and they’ll tell you drug abuse was a problem here long before the Opana abuse started about five years ago. Back in 2001, a chubby-cheeked 12-year-old with blond streaks named Whitney was given an OxyContin by her uncle in the parking lot of an Austin bar. She got hooked. Dealers didn’t care that she was 12. “Didn’t matter what age you were. They sold to kids, so long as you had the money,” Whitney, now 27, recalls.
That’s not big news though. This rural, tree-lined community 30 miles north of Louisville, just off Interstate 65, is a one-stoplight, one-truck-stop, one-physician community. Secrets don’t endure here. Everyone knows. Everyone knew. Dr. Tom Friedan, director of the federal Centers for Disease Control and Prevention, estimated that as many as 10 percent of Austin’s 4,200 residents inject drugs, mostly liquified Opanas.
In January, a pregnant woman from Scott County, where Austin is located, tested positive for HIV, the virus that causes AIDS. She named people she had shared needles with. Soon there were six, then 11 positive cases. Panic set in. The Indiana State Department of Health and the CDC came to Scott County, a pastoral setting that’s home to about 24,000 people. Disease-intervention specialists started tracking down hundreds of users. In March, Gov. Mike Pence declared a public health emergency. The number of HIV-positive cases continued to climb — 80, 140. Reportedly, one man named 57 people he’d shared needles with. “People are poor here,” one woman tells me. “We share everything.” The thinking went: I share blood with my brother, so why can’t we share needles? You could buy a used needle for $5. Some were reused hundreds of times, until they snapped in the arm.
By June, the Southern Indiana outbreak reached 169 HIV-positive cases, more injection-drug-caused cases than occurred in all of New York City last year, according to the CDC’s Friedan. It is the largest HIV outbreak in Indiana history, and CDC officials can’t recall anyplace in rural America that has recently experienced an epidemic of this magnitude. Normally Scott County sees five or fewer new HIV cases a year. (Just a handful of the 169 cases have been traced to surrounding counties.) Nationally, about 8 percent of new HIV cases are attributed to injection drug use; here, 90 percent of positive cases are linked to sharing dirty needles. Many who are infected don’t want to talk about it, sometimes speaking of their “status” in whispers. “I thought it was just a homosexual disease,” a tearful woman told the New York Times after learning of her positive diagnosis.
It all seems misplaced, seems like San Francisco in the 1980s or a third-world country. HIV, a disease that damages the immune system and is passed through blood, semen or vaginal fluids, is an urban problem. In 2013, only six percent of the diagnoses were in counties with fewer than 50,000 people. And Austin, the epicenter of this outbreak, carries honest grit, the kind country towns take pride in. Packed pews spoil the heavens on Sunday mornings. Hard-working men and women report to one of the handful of factories nearby for 12-hour shifts, sometimes six days a week. Lawnmowers hum ahead of a summer storm. Main Street has the staples — hardware store, bank, pharmacy, doctor, trains that crawl and clatter. And two major roads — one stretching north and south, the other east and west — siphon the traffic from narrow, residential side streets. A recent 30-year Austin High School reunion brought together a scientist, a dentist, a lawyer, but they all had long since moved away. It is a place that could easily be plucked from Alabama, Missouri, Kentucky, exalted in Americana lore.
This spring, as Austin stumbled into the headlines, the righteous sought light. Pray for Austin. Pray for Scott County. Let us unite, walk with our brother and sister, and heal the suffering.
Twenty-five percent of Austin residents live below the poverty line. Three-quarters of Austin’s elementary school children receive free or reduced-price lunch. In 2013, the Scott County Department of Child Services removed 117 kids from their caregivers, with 65 percent of those removed because of substance-abuse issues in the home. According to recent U.S. Census data, in Scott County one out of five adults lives in poverty, 22 percent have not graduated high school and 15 percent of the population is unemployed. The county consistently ranks at the bottom of Indiana’s 92 counties when it comes to life expectancy and overall well-being, according to the Robert Wood Johnson Foundation’s national health rankings.
In the early ’80s, John Cougar Mellencamp shot scenes for his “Pink Houses” video in Austin. It flexes like a patriotic anthem. Politicians use it to pump up crowds. Mellencamp grew up just 19 miles north of Austin in Seymour.
There’s winners and there’s losers
But they ain’t no big deal
’Cause the simple man, baby
Pays for the thrills
The bills the pills that kill.
I head to Austin for the first time in late April. Most homes — from tidy to ragged — warn outsiders with “No Trespassing” and “Private Property” signs. About 30 modest, one-room churches, many Pentecostal, dot the town. And cottony weeds — the ones wishes blow to bits — form soft, thick mobs at abandoned homes and the city ballpark.
Everyone who dips into the crisis — journalists, social workers, government health specialists — rationalizes the matter. Austin had the right ingredients in place. So do other rural communities — poverty, scant social services, no drug-detox or addiction-treatment facilities.
 |
| Tammy Breeding and her daughter sit on their porch on a quiet May evening in Austin. |
My first stop is the Indiana State Department of Health’s weekly media gathering at Austin City Hall. Quite formal, there are sign-in sheets, neat rows of soft blue chairs for reporters, a designated front-and-center space for television cameras, a podium where one message repeats: It’s a long-term problem, no easy fixes. The briefings occasionally end with a swatting of rumors: “I’ve heard of people becoming infected by stepping on needles. Is it true?” False tales fly among Austin residents. The wildest one overheard: Infected child bites innocent kid at daycare. Victim now positive.
By April, ISDH has set up a Community Outreach Center (dubbed the One-Stop Shop) in a large warehouse that looks out on I-65. Open daily, those who’ve tested positive can receive HIV antiretroviral medication here that tames the virus. The center offers prevention and substance-abuse information. People can sign up for the state’s affordable health plan. And thanks to an executive order from Gov. Pence, Indiana’s first clean-
needle exchange occupies a back corner of the warehouse. Pence, a Republican, previously opposed such exchanges. But he knew HIV would continue to spread if dirty needles stayed in the hands of IV drug users. (This spring, Louisville also started a needle-exchange program, in part due to the outbreak in Indiana.)
On press-conference days, SUVs parading news logos saturate Austin streets, hunting for fresh angles, dirty needles in trashcans and someone willing to shoot up in front of them. It’s not just local media. CNN, Yahoo! News, Al Jazeera, New York Times, Washington Post have trekked to Southern Indiana. By late spring, residents in the drug-addled parts of town have grown so wary of reporters that they honk to signal one another when one is spotted.
Tammy Breeding is a willing and early media regular — concerned single mom, quick with the sound bite. She’s known for the 9mm Ruger she carries on her hip and her front-lawn sign: No loitering or prostituting in front of or around these premises. A 41-year-old with feathery blond hair and intense blue eyes, Breeding is a former Hanover, Indiana, cop and veteran with a dial set to justice.
I meet her on a sunny May afternoon. She wears aviator sunglasses and a short-sleeve shirt rolled up to display a Marine Corps tattoo on her biceps. She moved to Austin a year ago from Fort Knox after splitting with a cheating fiancé. A Scottsburg native, she knew Austin had a bad reputation. But it’s affordable, so she and her three youngest children settled into a white house with a red roof on Austin’s north side. I’ll visit a couple times. It’s usually pretty quiet. The kids ride bikes in tight loops under her watchful eye and scale trees when she’s not looking.
Breeding says to look closer. “See that guy?” she says, pointing to a young man in black shorts pushing a lawn mower. “You can see the marks on his legs where he shoots up.” She sits on her porch, which communicates a set of values — American flag, spring flowers and security-camera signs. Breeding points to a house behind her. Drug house, she says. The one a half-block to the right? Drug house, with a vocal resident. “He was out last night calling me a bitch and all that,” she says. “Raising all kind of Cain.” Breeding frequents the Scott County sheriff’s website, investigating the names of locals booked into jail. She says her proactive, protective nature has made her an enemy. One prostitute tried to start a fight with her, she says. Another flashed her 12-year-old son. She has saved hundreds of iPhone pictures of suspicious cars and girls she adamantly believes are prostitutes walking her street. She shares them with police. But they have an “I-don’t-care attitude,” she says. “It’s gotten to the point that I’m ready to move.”
Down the street, shouts erupt. A car’s tires screech before speeding away. “See what I have to deal with?” Breeding says, sighing as she lifts her shades and peers at a worn, wood-frame house notorious for its drug activity. “He just got out of jail,” she says, referring to a bulky, bald man. About an hour later, the same man angrily waves a yellow car into the drug house’s driveway. More shouting. He tugs at his shirt, advertising fight mode. His fists punch wildly in the air. He hurls something at the porch — pop! — and stomps down the street.
A few houses down from Breeding, an elderly couple, Bill and Linda, watch it all from their porch swing. A school-aged brunette girl the couple watches after school twirls, uninterested in the commotion. Tanned, with shaggy gray hair, Bill says he and his wife have lived here since the 1970s. They’re not leaving the neighborhood. They were here first. Linda tends with a pile of mail on her lap. Bill drinks a glass of cola. They’ve grown to like the winter, Linda says, when trouble stays mostly indoors.
An Austin police officer stops in front of the house that has since quieted. He chats with a young woman in a tank top out front and leaves. “Typical,” Bill says. If such nonsense comes on his property? “I’ll kill all of them,” he says. “Gut ’em in my yard.”
A shirtless man with jeans sagging at his hips and a cross tattooed on his left shoulder waves Brittany Combs down on a pristine May afternoon — blue skies and breeze as pleasant as a purr. Combs presses the brakes of her white SUV with Scott County Health Department magnets on each side. The trunk is full of 1,000 clean, packaged needles and a dozen or so red “sharps” containers for dirty needles. Combs is 37, Scott County’s public-heath nurse. She’s also the face of this county’s mobile needle exchange, a weekday service she spearheaded after noticing residents were nervous about going to the Outreach Center for clean needles.

Scott County public-health nurse Brittany Combs delivers food to participants in the mobile needle exhange.
She hops out of the car and bends down to stroke a yapping dog. A mother of two small children and many animals, she can’t ignore pleas for attention. The shirtless man walks up to Combs with a limp in his step and a grin on his face. “I missed you guys yesterday,” he says in a voice that croaks. Combs is friendly, with a pretty smile and no-fuss look — curly brown hair tied back, glasses, no makeup. The regulars on her route perk up when they see her. “She helps me,” they’ll say to skeptical friends or relatives. Combs grabs a clipboard with a mandatory questionnaire.
“How old are you?”
“Forty-three.”
“Opana?”
“Yeah.”
“Hep C Test? HIV test?”
“Yup.”
“You sharing needles?”
“Hell, no.”
“Good. That’s what we like to hear.”
The HIV outbreak frightened people. They still do share needles, but only if they’re out of clean ones. Law enforcement has agreed not to arrest anyone with needles from the exchange. As long as they have the laminated white card showing they’re enrolled in the program.
A teenage girl in a gray tank top watches, listening to the man answer Combs’ questions. She sits on a loveseat parked outside, cushions askew. “How many times a day (do you use)?” Combs asks. “At least three,” he says. “Maybe more.” The girl seems bored, like this visit registers at about the same interest level as the mailman’s. “It’s just how they were raised,” Combs will say later. “It’s just normal.” The teenage girl’s eyes drift over to a Time magazine photographer also along for the ride who clicks photos of a skinny gray cat and a barn stuffed so full a dirty mattress hangs out like a tongue.
Combs hands the man a brown bag given to all needle-exchange participants. It’s stuffed with a flier indicating hours and services at the Outreach Center, a sandwich baggie with alcohol swabs, Band-Aids and cotton balls, and a brochure listing treatment and support groups in Southern Indiana. Most of the facilities are not in Austin. The closest residential drug detox and rehabilitation center, Turning Point, is in Jeffersonville, Indiana, just across the river from Louisville.
In hindsight, this HIV outbreak doesn’t surprise Combs. In 2011, Scott County saw 19 deaths from prescription-pill overdoses, about half of all deaths referred to the county coroner that year. Rates of hepatitis C, a potentially deadly blood-borne disease contracted mostly through needle sharing, had been climbing. Combs contacted other counties about the spike. “We were all seeing it,” she recalls. Other states, including Kentucky, Tennessee and West Virginia, had seen hepatitis C cases triple from 2006 to 2012. It seemed more trend than red flag. (Eighty-six percent of HIV positive individuals in the Southern Indiana outbreak are co-infected with hepatitis C.)
At first, people didn’t trust Combs. Thought for sure she was in with the cops. With that government-issued white SUV? Really, they didn’t trust any of the new faces filtering in from out of town. “We were joking when all this stuff was happening, they was gonna just put a big bubble around Austin and nobody’s gonna get out and nobody’s gonna get in,” one local woman told me.
Combs has found helpers on the street. Jerry Pennington, an outgoing, avuncular 56-year-old, has recruited friends into the needle exchange. After testing positive for HIV, he now persuades those who are reluctant or anxious that it’s best to find out. Pennington is red-faced with a gray beard, spongy nose and legs as thin as saplings. Combs knew she could rely on Pennington when he collected and turned in the “Chicago” needles. Early in the outbreak, an agency from Chicago passed out hundreds of clean needles. Since that was before the state-sanctioned exchange, those needles weren’t legal.
Pennington moved to Austin in the ’70s from Eastern Kentucky, which was about the same time he started shooting up cocaine. He’s lost three wives. “Every time I marry one, they die,” he says. Work came and went in factories until this past fall when his failing lungs sidelined him. On bad days, his breaths amount to feeble, hissy gasps. He now lives in a gray trailer with no electricity and the words “I love you” in black ink on the front rail.
One afternoon, Combs thought she spotted two of Pennington’s buddies injecting beneath his shade tree. She parked her SUV, and they scattered. As she gathered some clean needles for Pennington, he ran inside his trailer. “I have something for you for being such a nice lady,” he said, handing her a stuffed Winnie-the-Pooh riding a green elephant. The toy sits in Combs’ trunk, a constant companion on the needle exchange.
Combs continues her drive through Austin’s north side, a neighborhood known for drugs and poverty. A near-perfect grid of about a dozen blocks with seven cross streets, many homes look arthritic, exhausted. Only half of Austin’s homes are owner-occupied. Listen to talk on the streets — two or three landlords in town get labeled slumlords. On the north side, people walk at all hours. (One probation officer compared it to a college campus.) There’s no reliable public transportation in Austin. Few people have the money to purchase cars. Or their licenses are revoked, tagged with massive fines.
It’s late afternoon and a raw sewage smell stains the air — fumes from Morgan Foods, a canning plant that’s been around for 100 years and remains the city’s largest employer. Supposedly, on the days workers can sauerkraut and greens beans, the pungent smell thickens. (Neighboring towns came up with the nickname “Austink.”) Combs rolls past Tammy Breeding’s house. Breeding glares at the SUV. “I’ve been nothing but pleasant to her,” Combs says with an exasperated laugh. “I don’t know what her problem is.” The day before, Breeding had told a Louisville news station that a recent decision by the state health commissioner to extend the needle-exchange program for a year was a big mistake. “Give them the drugs too,” she said. Combs was originally also against the idea. On one of the first few days of the exchange, she handed needles to a mother who chuckled at her daughter passed out on their kitchen table. “I’m like, ‘Oh, my God, what are we doing?’” Combs recalls. But research proved convincing. Needle exchanges stop disease transmission.
 |
| Jerry Pennington stands outside his home after a visit from Scott County's mobile needle exchange. |
Combs heads to Scottsburg, four miles down the road, to check on a couple recently evicted from their Austin home. “I knew we had couch-jumpers in this community, but I didn’t know it was this bad. Like, literally I find people in different houses every time I see them,” Combs says. “They have nowhere to live.” She pulls up to a compact apartment complex in the shadow of Scottsburg’s water tower.
“Who is it?” a woman yells.
“Needle exchange!” Combs replies.
The woman opens the door, spots the Time photographer and cups her hands over her face. A short, thin man with a military ball cap follows suit. “I’m serious,” he warns. “I’m schizophrenic bi-polar.” Later, he’ll tell his story in what seems like one memory that runs 30 minutes long — his father committing suicide, a violent childhood, his sister’s death from a dirty needle, the way Opanas calm his demons. “No pill has helped me as much,” he’ll say. For now, he heads to the trunk of the SUV. His limbs fidget but eyes rarely blink.
“How often do you shoot up?” Combs’ partner on today’s needle exchange asks.
“Every second of the day if I can get it,” he says. “I’ll take 140.” That’s the maximum number the needle exchange will give out in a week. A chart on the back of the clipboard shows the math — 20 injections a day.
The exchange has three sizes of needles — 27s, 29s and 31s. The bigger the number, the thinner the needles. To me, they all look the width of sewing needles. The 27s can hurt, but shooting liquefied Opanas typically takes a larger-gauge needle. That can increase tissue damage, heightening the risk of HIV transmission. (Opanas used to be crushed, mixed with water and injected. In 2012 Endo Pharmaceuticals, the makers of Opana, introduced a version of the pill that was supposed to cut the risk of abuse due to a new coating. But users still can cook it down into a liquid.)
The woman who answered the door agrees to talk if we call her “Nicole.” She’s 28 years old, with green eyes that rival the Northern Lights. Her mom had a brown eye and green eye. “Grandma said one looked for trouble, the other looked to heaven,” Nicole says.
She plops into a wheelchair and grabs a newspaper to color in letters like bubbles on a multiple-choice test. She occasionally picks at a dark, caterpillar-like scar on her right arm. It’s a nervous habit. Her sister introduced her to pills as a teenager, and Nicole liked the high. But they also helped with chronic neck pain, a result of getting hit by a car while walking on a country road. Nicole has quit pills in the past. Once while serving time for robbery. But the relapse rate for opiates is about 85 percent. “I’m real weak-minded to everything,” she says. “When I lose somebody, I just give up.” Both her parents died while she was incarcerated.
Nicole’s a well-known figure in Austin. And at the Scott County courthouse. She has shuffled in zebra stripes across the Scottsburg town square from the squat jail to the handsome brick courthouse many times, wrists in cuffs, chained in single file to fellow inmates. Nicole points to a tattoo on her right foot that she got during one stint in jail — Loyalty. Her pal used staples from their court papers and melted checkers to mark them with matching ink.
It’s estimated that about 80 percent of Scott County’s inmates have been arrested for drug-related crimes, including theft and prostitution, two ways to scrounge up money for pills. Nicole has a court date in a few weeks. She says her probation officer found drugs on her. While she’s enrolled in the needle exchange, that doesn’t make drugs legal. (Even sanctioned needles give law enforcement enough probable cause to search.) Nicole throws a cigarette butt into a trashcan a body length away. She wants to get sober, she says. Instead, on July 7, a month after we talked, booking will snap her mug shot — green eyes round and frozen, a tired pout. Back in jail.
Donald Spicer, Austin’s police chief, stands as wary watchman to the justice system’s revolving door. “It’s the same people I was dealing with six or seven years ago,” he says. We are having lunch at a Huddle House, one of Austin’s two restaurants. Aside from a handful of gas stations, it’s one of the few places to grab food. Austin’s only grocery store shut down a few years back. (The closest one is in Scottsburg.) Spicer fits the part of small-town chief — trim gray beard, and a 46-year-old’s round, soft shell buttoned into a pressed navy-blue uniform.
Spicer opts for the country-fried steak.
“Mashed potatoes?” our waitress asks.
“Yeah,” Spicer replies.
“Gravy?”
“Yeah.”
“Green beans?”
“Green beans are fine.”
The law-abiding majority of Austin fumes at those who commit crime, rinse and repeat. The county is spending $15 million to renovate and expand the jail just to fit them all. Spicer’s an easy punching bag. Even a 15-year-old Austin girl told me, “I think the authorities could be tougher.”
Last summer a new Indiana law softened penalties associated with thefts and low-level drug-related charges. Many drug-possession charges that used to be felonies are now misdemeanors. Mandatory minimum sentences on drug offenses were abolished. (In Kentucky, possession of most controlled substances is a felony.)
Jason Mount, Scott County prosecutor, says misdemeanors can, of course, still result in jail time, but, he says, “If you’re a user and we arrest you, and you have at most 182 days you can spend in jail . . . the only way we’re going to get you to do 182 days is if we try you, and no county has the resources to try every misdemeanor.” So plea deals are made — a couple months in jail, maybe rehab.
Mount says that “revolving door” criticism “sets me off.” He points to data showing that, per capita, Scott County sends more people to prison that any other county in Indiana except one. And he says the county’s two judges routinely set high bonds. The Indiana Department of Corrections pushed for the law change to clear overpopulated prisons of low-level criminals. Mount says it’s now mostly up to counties to come up with alternatives, perhaps rely on probation more. But Scott County’s probation department is swamped as is. Five officers each have about 300 cases. The recommendation is 100.
Spicer finishes his meal, leaving most of the green beans. His two-way radio squawks: “Call in, please. It’s an emergency.” He sighs. “Everything is an emergency to some people,” he says.
He calls the number dispatch gives him. “This is Donald Spicer — what’s going on?” he says into his cell phone. “Yeah, yeah, yup. I’d heard about it.” He patiently listens to a concerned father whose daughter just started using. “It’s crazy. That’s the street value of them now,” Spicer says. One Opana can cost anywhere from $30 to $200. When Opana first swamped Scott County, they obtained them through prescriptions or relatives with prescriptions. They were easy to get from doctors leaning on pain pills as a quick fix to chronic pain. (Since 2007, two pharmaceutical companies have pleaded guilty to criminal charges that they misled doctors into believing the drugs were safe.) One couple that received pills from an aunt admitted to shooting up $2,000 worth of pills in a day. Now, most of the Opanas are trafficked in from other counties and states. (Unlike urban areas, heroin has only made a small appearance in Scott County. Meth remains problematic.)
The man asks Spicer to talk sense into his daughter. “We’ll look into it,” the chief says. Spicer speaks slow and mellow. The tone could be mistaken for indifference, a man ready to trade out a badge for a fishing pole. (He owns a small bait shop in town.) But he grew up just a few blocks from this Huddle House, in a neighborhood known as Spicertown. A great-uncle still lives right near the ditch that, as a child, Spicer and his buddy would plunge their bikes into after a good rain. Closest thing to a splash park.
We head to Spicer’s impeccably clean black Dodge Charger to ride around Austin. Spicer’s fingers occasionally swipe off inconspicuous dust on the dash.

Austin police chief Donald Spicer rides around his hometown.
He’s quick to share his main challenge: Austin has six officers. That basically amounts to one cop on duty every shift. “Current federal statistics say (you should have) 2.3 officers per 1,000 (residents) . . . just to maintain the law,” he says. That would add up to about 10 officers, four more bodies than he has now. Spicer has no detectives, no special drug unit. Indiana State Police and the Scott County sheriff help when they can. At one time, Spicer had eight full-time officers and two part-time. But that federal grant dried up.
Growing up, he says, marijuana and cocaine were the drugs he heard about around town. The pain pills came “about 16 or 17 years ago,” with OxyContin leading the way. He started at the department as a volunteer officer 20 years ago. By the time he became chief in 2002, he knew there were problems. He watched a former high school classmate turn to prostitution to afford drugs. People were demanding pills from Scott County Memorial Hospital’s emergency rooms and holding up pharmacies. “One of the first things I did as chief . . . was to eliminate us taking reports of stolen medication,” he says. People who reported they’d had drugs stolen would “take the police report back to the doctor (to get more drugs). Well, we picked up on that very quickly. They were trying to use us to get drugs.”
Spicer drives down Main Street and points to a young brunette in jeans and a hooded sweatshirt, a gas-station soda in hand. “There’s one of our prostitutes. She has a nickname — ‘Polar Pop,’” he says. “Seriously.” Spicer hopes to hire a seventh cop by the fall. Austin’s tax base doesn’t give him a lot of wiggle room in the budget to cover the $35,000 salary. People go to Scottsburg to grocery shop, Clarksville to dine out. Multi-million-dollar Morgan Foods sits right across from the police station but technically isn’t in city limits, so it pays no city taxes. “Not enough money to go around,” Spicer says.
We pass a trio lingering on the side of a street on Austin’s north side. “They are up to something no good,” he says, pausing. “But — that’s not enough to arrest them.” As he drives, Spicer seems drained, a bit troubled. Spotting a home that looks inside out — broken appliances, furniture and scrap on the porch — he quietly says, “You can’t fault somebody for being poor.”
He wrestles between compassion and logic. “They’re making choices,” he says, referring to drug use. “They choose to do it.” But one of his daughters was addicted to meth. “I’m not proud of it, being a police officer,” Spicer says. “But the point is it doesn’t matter what kind of money you have or what family you came from. If you make the wrong choice, you can be on the wrong side.” He says his daughter has completed a lengthy rehab and is better now. But Spicer now understands that addiction is a chronic disease, that it alters brain chemistry. It seizes judgment and behavior parts of the brain. It can take months or years of sobriety for the brain to fully recover. “It’s a monster, really,” he says.
On a humid May evening, a faithful crowd packs into Grace Covenant Church on Main Street. From the pulpit, pastors energize. “Father, tonight we pray that you will expose anything that is not right in this community, and not just expose it but expose it by name!”
“Yes, yes!” The crowd rejoices. Hands lift. Hundreds of heads nod. People have wandered. HIV arrived for a reason.
“God has allowed this to happen for his own personal benefit, not just for the people in the streets to come back to him,” a young man preaches. “This is for us! We’ve been apathetic. We’ve been slow and weak in our regards to Christ.”
“Amen, amen!”
The congregation exits. Tonight is the weekly prayer walk. A mass of bodies, as wide as the street and longer than a city block, walk into the sunlight and throughout Austin. A man who leads blows a shofar, an ancient instrument traditionally made from a ram’s curly horn. Often used to proclaim spiritual warfare, the mournful wail silences the crowd. Hands join. Eyelids collapse. Some mumble. Some announce.
“This is the change we really needed.”
“God, expose sin! Expose the darkness!”
A pamphlet offers guidance. On Factory Drive, ask for “God to awaken the mindset of the people from that of poverty and laziness.” On Wilbur Avenue, pray for “God to shine the light of the gospel in the hearts of those that live with deep depression, anxiety, fear and many demonic strongholds.”
Manchester, Kentucky, inspired the walk. Known as the “Pain Killer Capital” of the nation in 2004, churches united, staging a march of thousands of concerned citizens. The message to drug dealers: repent or go to jail. Improvements followed. Faith-based drug-recovery programs popped up and local politicians helped secure federal money for a residential treatment center. Manchester now calls itself the “City of Hope.”

A trembling string of notes rings — “yo lo lo lo lo lo” — as a man prays in tongues. The shofar will blow again, indicating time to walk to the next prayer stop. Christian music will play from speakers propped in an infant stroller. But before the procession, a final plea. A blond, middle-aged woman lifts her head to the sky. Tears streak her cheeks.
“Why in this county, God? Why?”
Scott County’s history reads like industrious Midwestern fare. A group of Kentucky Baptists were among the first white settlers in the early 1800s. Other pioneers followed, mostly from the South. Hard-drinking Irishmen built the railroad and Austin’s town center bustled. By 1870, Austin boasted four doctors. Today there is one.
The story goes that veterans of the Mexican-American War named Austin in honor of Austin, Texas, where many of them were stationed. By the early 1900s, advances in technology led some young entrepreneurs to start the canning plant that is now Morgan Foods. Mostly, they canned the region’s abundant tomato crop. The first and second world wars brought such great demand for canned food, a joint factory that has since moved its operations supplied the cans to Morgan and Austin became known as the “Canning Capital” of Indiana.
One afternoon, at a park across from Morgan Foods, I meet a jovial, burly grandpa feeding ducks with his two-year-old grandson. The man colors Austin’s history differently than the library books. “Austin’s always been rough,” he says. “Back in the ’70s, they called it ‘Pistol City.’” People took the law into their own hands.
Part of that was the culture brought here straight from Appalachia, he says. In the 1950s, Eastern Kentucky coal jobs plummeted by more than half, and families fled for factory jobs in Michigan, Ohio and Indiana. “Austin was as far as they could get on one tank of gas,” goes the joke. The man loops his lesson to present day. The addiction, that’s Appalachian too. Moonshine in the mountains, drugs here, a curse that crossed state lines. Many lifelong Austin residents echoed this theory to me.
But other communities incubate similar environments. The last town to experience an HIV outbreak similar to Austin was Belle Glade, Florida. Between 1982 and 1986, 62 people contracted HIV and ultimately AIDS through IV drug use and sexual contact. Most were black and poor. A 1985 New York Times article described Belle Glade as a “farm community long locked in penury and squalor. . . . Diseases of overcrowding, poor sanitation and malnutrition have long been documented.” (The area continues to have high HIV rates.)
In Austin, families discovered a cheap place to relocate just off the interstate. Relatives followed grandparents and uncles who managed life through relatively stable factory work or a government check. Blood brought a big part of Austin together.
Whitney and David Richie live on Austin’s west side, another troubled neighborhood. On the front door of their rental home, they’ve posted a sign in red ink: No knocking 9-10. The nighttime hour is “when most of the junkies are out,” David explains as he rolls his own cigarettes on a cookie sheet in their wood-paneled front room. It’s a dark, busy space — a Confederate flag on one wall, more than a dozen framed family photos, including one of Whitney and David cheek-to-cheek in a car, mid road trip. Above David’s head, a poster of a couple kissing on the beach sits next to a street sign: “S. High St.”
Longtime drug users, the couple says Dec. 21 was the last day they injected Opanas. Both have quit with the help of Suboxone, a drug that blocks opiate receptors, shutting down cravings. It’s considered safer than methadone (which can become addictive) and is now more widely used. David pulls out a packet to show the medication that looks like a breath-mint strip. “She don’t get out of bed until I have her strip open for her,” David says, referring to Whitney.

Whitney and David Ritchie at a food pantry in Scottsburg.
Whitney’s Suboxone prescription is running out. After that, it’s up in the air. “Take a chance or die, I guess,” she says. “Or relapse.” Her current doctor won’t accept the health insurance plan she got through the state. A few others she has contacted demand cash (not uncommon nationwide because of low insurance reimbursements for the office visit), and she can’t afford that. Many physicians won’t prescribe Suboxone, one reason being that it sells on the street for about $25 a strip, often to people trying to sober up on their own. Dr. William Cooke, Austin’s sole physician, offers Vivitrol, a monthly injection that suppresses cravings. But Vivitrol doesn’t have the hint of opiate that Suboxone does. So patients experience withdrawal.
David was 14 when his dad, a “biker,” sat him down and “put a pound of weed down in front of me and told me, ‘Learn how to bag your own bags; have my money by Friday.’”
“A lot of families are like that,” Whitney chimes in. Her last school photo from the sixth grade — of her smiling and holding a basketball — stares from a perch on their television. She says she has “no good memories” from growing up in Austin. Her parents battled addiction. Electricity was periodically shut off. She dropped out of school barely past the elementary years.
“And that’s how I grew up,” David says. “I quit school. I’m a waste. I’m very intelligent. I could sit down in front of a computer . . . take it apart and put it all back together.” The 39-year-old looks hardened, a bandana often tied around his head. Tattoos cascading down flesh — spider webs on his forearm, a Harley-Davidson symbol with his mom’s name on his hand, a mad scientist on his leg and two Voodoo dolls (one for each ex-wife) on his thighs.
Whitney and David talk about their lives for hours. They’re among the few in Austin who invite media in. Maybe their story can help others, they say. For weeks, the photographer for this story and I have been introduced to others struggling with addiction. Most shy away or vanish.
On a hot June afternoon the photographer and I go with Whitney and David to a Scottsburg food pantry, a maze of cheery yellow walls and green shelves. Whitney pushes the cart through narrow aisles. Her long brown hair is pulled up. She wears sparkly sunglasses, jean shorts and a swipe of cherry ChapStick. Twenty-seven years old, she still hasn’t outgrown childlike, plump cheeks. David hugs his petite wife’s shoulders, hanging on as they walk in step. The two are like magnets, always close. Nine years ago, about the time they got married, David tattooed “Whitney + David” on Whitney’s left hand.
On the way to the pantry, David and Whitney giggle recounting their love story. David started crushing on Whitney when she was just 13. The saga veers Merle Haggard: David goes to prison, his then-wife winds up with Whitney’s boyfriend. They marry soon after Whitney’s 18th birthday.
A pantry volunteer pulls chicken noodle soup, melon, frozen vegetables and a red velvet cake from shelves, stacking all of it in the cart. Without this place, groceries would be hard to afford. The two briefly worked at the same auto-parts factory a few years ago, but Whitney says her painful sciatic nerve problems and eczema couldn’t handle the hot, laborious job. David can’t get hired full time anywhere. When companies do the background check, they find his criminal record, including drug possession and a conviction in the late ’90s for child molestation. They rely on Whitney’s disability check and an informal pawn operation they run out of their house for money.
Until six months ago, David says, he also cooked meth and dealt drugs. But that lifestyle soured their love. David was accusing Whitney of prostituting. Fights exploded. They considered signing up for inpatient treatment. (After the HIV outbreak, Turning Point in Jeffersonville gave priority to folks from Austin, reducing wait times for one of the 18 beds in half.) But that would’ve meant being apart for 30 or more days. “I can’t be away from him,” Whitney says.
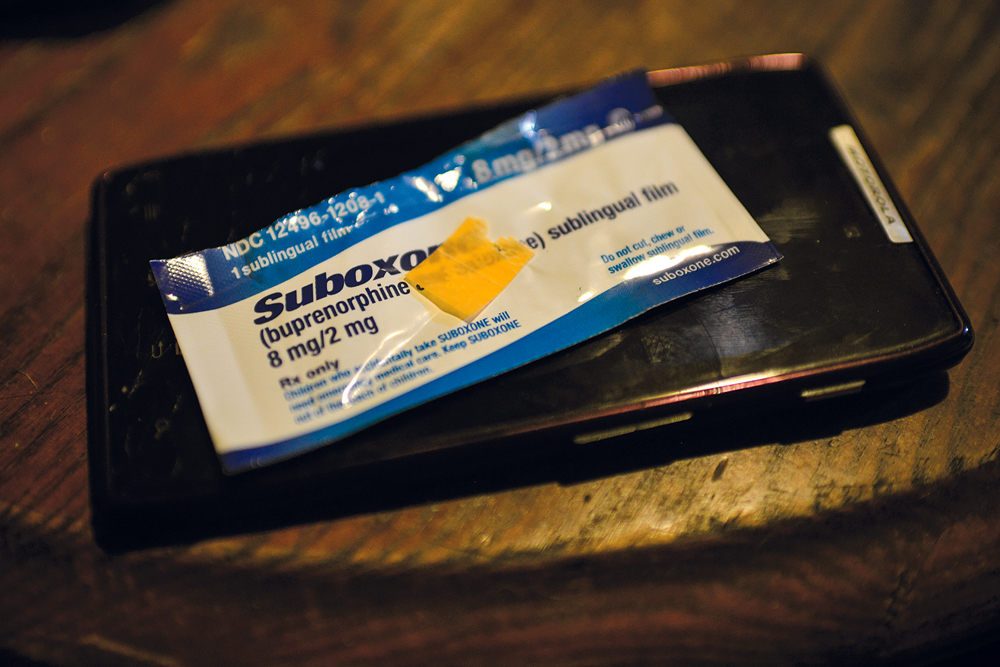 | |
| Half a strip of Suboxone, a drug that helps curb cravings for Opana. |
They feel lucky. Both have tested negative for HIV. Many of the people they shared needles with have not, including the last person they injected with. When this story went to press, 491 individuals were identified as possibly infected, 257 tested negative, 174 were positive; dozens of others either couldn’t be located or refused testing.
Back from the pantry, David turns on a Kevin Costner movie. A close friend, Josh, whom David calls his “brother,” seems disoriented. He places food in the sink. Josh’s skin appears sweaty, eyes glazed. David knows what’s up. He says Josh just shot up some Opana. The couple lets friends crash at their house and use drugs in a garage out back. Better than out on the street, they believe. Perhaps it’s a way to hold on to old ties. Friends don’t like it when friends or relatives get clean. “They’re afraid you’re gonna start talking to cops,” Whitney explains. The only rule is no drugs in the house. “If it’s in front of me, I’m going to do it,” David says.
A red suitcase lies on the floor. Josh has a ride to an Indianapolis rehab in four hours. About a month ago, he woke Whitney and David, pounding fists on their front door and windows. They rushed to the door and found Josh foaming at the mouth. David stuck him in a cold bathtub and held him for two hours. They didn’t call an ambulance out of fear cops might come too.
Someone knocks on the door. Josh leaves, says he’s going to the Outreach Center for his HIV antiretroviral meds. On the couch, Whitney burns through cigarettes, one after the other. They worry. Will Josh return or abandon rehab?
I ask them whether it’s hard for the newly sober to return to Austin.
“You’re gonna have to move the hell out of Austin,” David states.
“No, I don’t think so,” Whitney says. “David, you’re gonna tell me this town is gonna stay the same?”
David, who’d briefly left the room, returns agitated.
“Yeah, it ain't gonna change. Austin has always been this,” he says. “Austin has always been the number one drug capital of the Midwest. Like Gary’s the murder capital.”
“You’ll never leave Austin and I won’t either. I was born here. My family’s here. And if no one stays to try and help . . . what the hell is gonna happen?” Whitney says, taking a drag from her cigarette. But maybe David has a point. “Everyone in this town is gonna use something,” she says. “If it’s not Opana, it’s gonna be heroin or methamphetamine or coke.”
In the two months I spend in Austin, victories spring up. Twenty-five men enter the Salvation Army’s rehab programs in Indianapolis and Fort Wayne, thanks to the efforts of local churches. By late June, 12 individuals have completed Turning Point’s treatment program. The AIDS Healthcare Foundation, a California-based nonprofit, partners with Dr. Cooke’s office to increase HIV services and pays for a mobile testing van. Morgan Foods funds the salary for a drug detective in the sheriff’s department. Infectious-disease specialists from Indiana University will treat the 10 percent of jail inmates who are HIV positive. The local job-training office distributes 650 fliers advertising free job training and help completing the high-school-equivalency test.
Big plans are dreamed in silos. A treatment center in Austin. A virtual college campus. The city of Austin hires a woman assigned to get groups talking. She led the rebuilding efforts in nearby Henryville after their 2012 tornado. She cuts ideas down to reality. No windfall of money is coming. Nor should it, says Dr. Carrie Lawrence, a postdoctoral fellow with Indiana University’s Rural Center for AIDS/STD Prevention. “It can’t be top-down, here’s a bunch of money, fix it, and then 10 years from now, when budgets get tight, it’s gone,” Lawrence says. “That’s the norm we can’t seem to get away from.” (A Planned Parenthood clinic in Scott County that provided HIV testing and women’s healthcare closed in 2013 when government funding decreased.)
Lawrence says Indiana needs to create a culture where chasing funds for health-related issues is a constant, top priority. According to the Trust for America’s Health, Indiana ranks 37th in the nation for state per-capita health investment. (Kentucky ranks 15th.) When it comes to funding for HIV treatment and prevention, Indiana lags behind. The CDC and Health Resources and Services Administration are two major federal funding sources for HIV care. Indiana ranks 50th per-capita in funds received from those two agencies. “We have to stop being such a reactive society,” Lawrence says. “And waiting for something to happen and then saying, ‘Wait, we need to do something differently.’” At least in poor urban settings there’s some kind of pipeline one can enter when ready — homeless shelter to drug treatment facility to halfway house to job training site to the bus for their first day at a new job. Most rural communities lack that structure.
When he’s not juggling hundreds of patients, Dr. Cooke allows his mind to get out in the weeds, those puffy, cottony ones fit for wishes. Hope, that’s what’s missing, he believes. “It’s a very challenging area,” he says. “This particular group has been discriminated against for a long time. . . . They’re looked at as addicts, junkies. They’re looked down upon.” Cooke has read studies that show if people can follow a “sequence of success,” they have a very low chance of living in poverty and risking the spirals that culture can bring. “Graduate high school, get a job, get married, have a kid,” he explains. “Pretty simple stuff. But you have to do it in that order.”
By late June, Austin seems calmer. Weekly media briefings are over. A billboard 15 miles south of Austin encouraging HIV testing is gone. The Indiana State Department of Health holds a press conference in Indianapolis that feels like a finale.
Reporters receive an 11-page plan. ISDH will pay for another public-health nurse in Scott County, as well as care coordinators and disease specialists. Thanks to a one-year grant from Indiana’s Division of Mental Health and Addiction, an office with behavioral and mental-health therapists will open in Austin. LifeSpring, the company operating the office, hopes it can be financially self-sufficient once the grant expires.
A few days later, I ride with Combs on the needle exchange again. She says some of her regulars are uneasy. “People keep asking, where are you going to? What’s going to happen?” she says. The Outreach Center is scaling back. It will be open one day a week instead of every day and is relocating to a building right near the police station. Some in Austin are convinced cops will spy on who’s getting needles.
Combs’ needle exchange will continue four days a week. Right now, she operates with thousands of donated needles and a $10,000 grant. (She has dispensed more than 24,000 clean needles since the exchange began and collected about as many dirty ones.) Eventually, the county will have to cover most of the cost. Combs pulls up to Whitney and David’s house. Josh is on the couch. He only spent four days in rehab, long enough to detox. He hands Combs a sharps container full of needles. He’s using again. “Mostly because of this,” he says, raising a bandaged hand. He slammed it in a car door and needs something for the ache.
David walks into the room with another container. “There’s 45 (needles) in there. I don’t need anymore,” he says before disappearing to another room. (He’ll tell me later he’s not using Opana, just occasionally dissolving Suboxone in a soda can and shooting that.) Whitney sleeps through Combs’ visit. “That’s strange,” Combs whispers when back in the car. Usually, it’s social hour at their place.
Earlier in the day, Whitney lay curled up on her couch, under a white blanket and heating pad David had tenderly placed on her. Withdrawal symptoms had arrived. Her Suboxone strips had run out two days before.
Whitney texted Combs, seeking advice. Combs suggested an over-the-counter antidiarrheal. Whitney then texted a friend who has been withdrawing so bad she broke down and got an Opana. Her friend typed back. Whitney placed her phone on her chest, looked up at the ceiling. “Everyone’s just going to bed,” she moaned. “Trying to sleep it off.”
Combs is a bit of a snoop. As she drives through Austin, she passes out food or stops to chat, just so she can sense whether folks are taking their HIV medication and following through on promises of checking into rehab. Combs animates when talking about a recent success story. Of the 112 patients engaged in HIV treatment, 11 have gotten their viral loads so low they’re no longer contagious. “That’s just crazy!” Combs says, giddy at the progress.
Infectious-disease specialists from Indiana University were treating many of those patients. Her excitement flat-lines. “Now the infectious doctors are gonna leave,” she sighs. At one point, word was that IU was going to join forces with Dr. Cooke or open its own independent office. A disagreement of some kind between Cooke, the AIDS Healthcare Foundation (whom Cooke recruited to his office) and IU canceled those plans, leaving Cooke as the sole HIV treatment provider. A clinic run by University of Louisville Physicians in downtown Louisville is one of the only other options.
Combs heads for a two-story butter-yellow home where two sisters live. When she reaches the house, there are whispers: “The kids have been taken.” The sisters plea with Combs. They want rehab. “I’m going to be 25 in a few weeks,” the older sister, Tara, says. “What can I say I’ve accomplished? I got no kids yet. My (HIV positive) status — I’m ready to get my whole life straight,” she says. “I’m at rock bottom.”
Tara’s younger sister sits near a mattress where two kittens nap in yin-yang pose. Black-and-white photos of her young girls surround her. One of her long legs bounces anxiously. “I need to get in now,” she says, visibly upset that her daughters were taken from her. She’s hoping Child Protective Services will return them if she commits to a rehab program. Combs hands them pink slips indicating they’ve tested negative for tuberculosis, a requirement for inpatient facilities. Combs says in the months since the outbreak, “tons” more people are interested in sobering up. “It’s probably multiple things,” she says. “It’s that the HIV has scared them. It’s that we’re here to help and they didn’t know where to go for help before. They’ve grown to trust us. And police are cracking down, CPS is cracking down.”
There’s a knock at the door. It’s the sisters’ brother, who’s fostering the kids. Just off work and still in the white jumpsuit worn at a nearby factory, he asks about diapers. Tara’s younger sister runs to hug her toddler with sparkly blue eyes, cradling the child’s neck, delivering loving pecks on her forehead. As the children leave, a reminder to the brother in charge: “She has diaper rash!” The younger sister crumples onto the stoop, quiet and sobbing. Tara places an arm around her sister’s shoulder. “Everything happens for a reason, sis,” she says. “Keep your head held high.”
The June sky is the color of a bruise. Clouds burst, drenching the afternoon. Inside the Oasis of Hope Missions on Austin’s north side, Debbie Ousley sprays Lysol in a one-room chapel with white walls and plastic picnic tables sandwiched between 12 blond pews. “So mildew-y in here,” the 60-year-old mutters. Her husband Jerry slips Christian music into a boom box. “Too loud?” he asks.
“It could go down a little,” she replies as she pulls Styrofoam plates from a large red bin.
 |
| Debbie Ousley in front of the Oasis of Hope Missions, located on Austin's north side. |
For more than two years, the Ousleys have helped prepare a weekly free meal for those in need. Sometimes they feed 25, sometimes 125. At 4 p.m., a 15-year-old and her little brother walk in. Two women follow, piling fried chicken, hamburger buns and potato salad onto plates. The crowd is thin, so Debbie and Jerry head out to the streets. “We’ve thought about getting a dinner bell,” she says, laughing.
Gray-haired with a round, kind face, Debbie is the steely-soft type. She’s a hugger, tears up easy when talking about the “hurts” people in Austin suffer. But she won’t bend on her beliefs. Ousley has allowed the needle exchange to park behind the mission on meal nights. She knows drug deals play out feet from the chapel. “We’ve been accused of being enablers,” she says. “But Jesus said, ‘Feed him.’ Not: ‘Feed him because they deserve it.’”
With tables full, she picks up a microphone. “Test, test. Hi, everybody!” she says, before jumping into scripture. “You know what amen means? It means ‘let it be.’”
A man stumbles in, bounces from table to table and talks loudly. His eyes are as wet and stagnant as day-old puddles. He’s higher than Debbie has ever seen him. She breaks from her sermon, touches his shoulder. “You all right, buddy? You hungry? Quiet down a bit. You’re out-preaching me,” she says with a laugh. “Go ahead and get some food. We want you to get some food.” She grew up with an abusive alcoholic dad. Five siblings have died of cancer. She just got diagnosed with breast cancer. Empathy comes naturally.
A handsome 36-year-old named Enick walks in. Before he gets his meal he heads straight to Debbie to tell her he’s headed to rehab in Indy at the end of the week. “Wonderful,” she says. She wants folks to take advantage of opportunities that have come in HIV’s wake. “That’s one of my fears,” she says. “That when the dust settles, it will go right back.” She offers Enick gas money for the trip and gives him plastic bags of clothes and toiletries. She and other volunteers form a circle around him and pray.
Outside, the storm has lifted, leaving a cool breeze. Boys play basketball. Optimism seems to have choreographed the evening’s final moments. But Austin is still in the raw stages of healing, the part where no one knows the outcome. I find out a week later that Enick didn’t make it to rehab. He’s in the Clark County Jail because he failed to appear at a court date for theft and criminal-trespass charges. Hope can be such a task. Then I remember a quote Ousley leans on in cynical times: “If you’re drawn to broken birds, don’t be disappointed when they don't fly.”
"The Craving" originally appeared in the August 2015 issue of Louisville Magazine.
Click here to subscribe to Louisville Magazine.